 Hablamos Español
Hablamos Español
Low Grade Astrocytoma
This type of tumor is a benign version of the tumor glioblastoma multiforme. It comes to medical attention in a more subtle way, possibly with seizures, often with focal onset. This tumor may be hard to appreciate on imaging studies as it may not enhance with contrast administration and therefore may look similar to normal brain tissue.
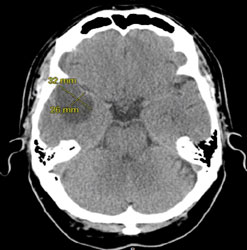
This CT scan shows a low-grade astrocytoma typically appearing less dense than the surrounding brain tissue.
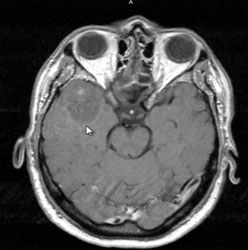
On MRI the low-grade astrocytoma looks similar to brain but frequently with less signal intensity, and the tumor does not enhance with the administration of intravenous contrast agent. This particular tumor was difficult in that it surrounded the middle cerebral artery. An attempt at complete resection of this Grade II astrocytoma involved skeletonizing the middle cerebral artery and taking out tumor involving the temporal lobe and the frontal lobe.
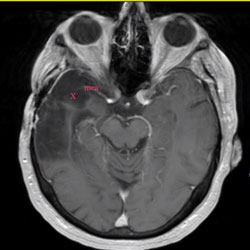
The MRI to the right is taken 6 years after initial treatment. There is no sign of any tumor recurrence. The x depicts the tumor resection area, and the middle cerebral artery is labeled mca.
While these are slow-growing tumors, their typical behavior is to undergo malignant transformation. This typically occurs 7 or 8 years or more from the time of diagnosis. This makes a case for consideration of aggressive treatment at the time of diagnosis. This allows potential cure before the tumor can become malignant. The challenge with these low-grade astrocytic tumors is that they appear very similar to normal brain tissue under the operating microscope. Surgery may be aided by utilizing technical strategies such as intraoperative image-guidance, intraoperative MRI (not widely available), awake surgery with cortical mapping, and use of frequent marginal biopsies to histopathologically examine the tissue. This allows as aggressive a resection as possible, with a minimization of damage to functional surrounding brain tissue.
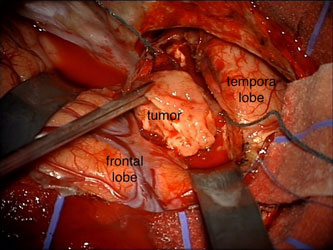
The photograph above shows a low-grade glioma being taken out of the anterior temporal lobe. The tumor color and consistency appear very similar to that of normal brain.